Have
you ever wondered why hypertension appears to be the primary driver
of COVID-19?
(Coming off ACE Inhibitors to start another blood pressure
medication can be hard to do without readily available medical care.
In the times of COVID-19 this will not be available in many areas of
the nation. One does not want to undergo a stroke or
heart attack based upon discontinuation of a drug because of a
controversy. Thus, ALWAYS consult your doctor.
It is however very prudent if you are on these medications to follow
strict social distancing, wear a mask and stay safe at home as much
as possible.)
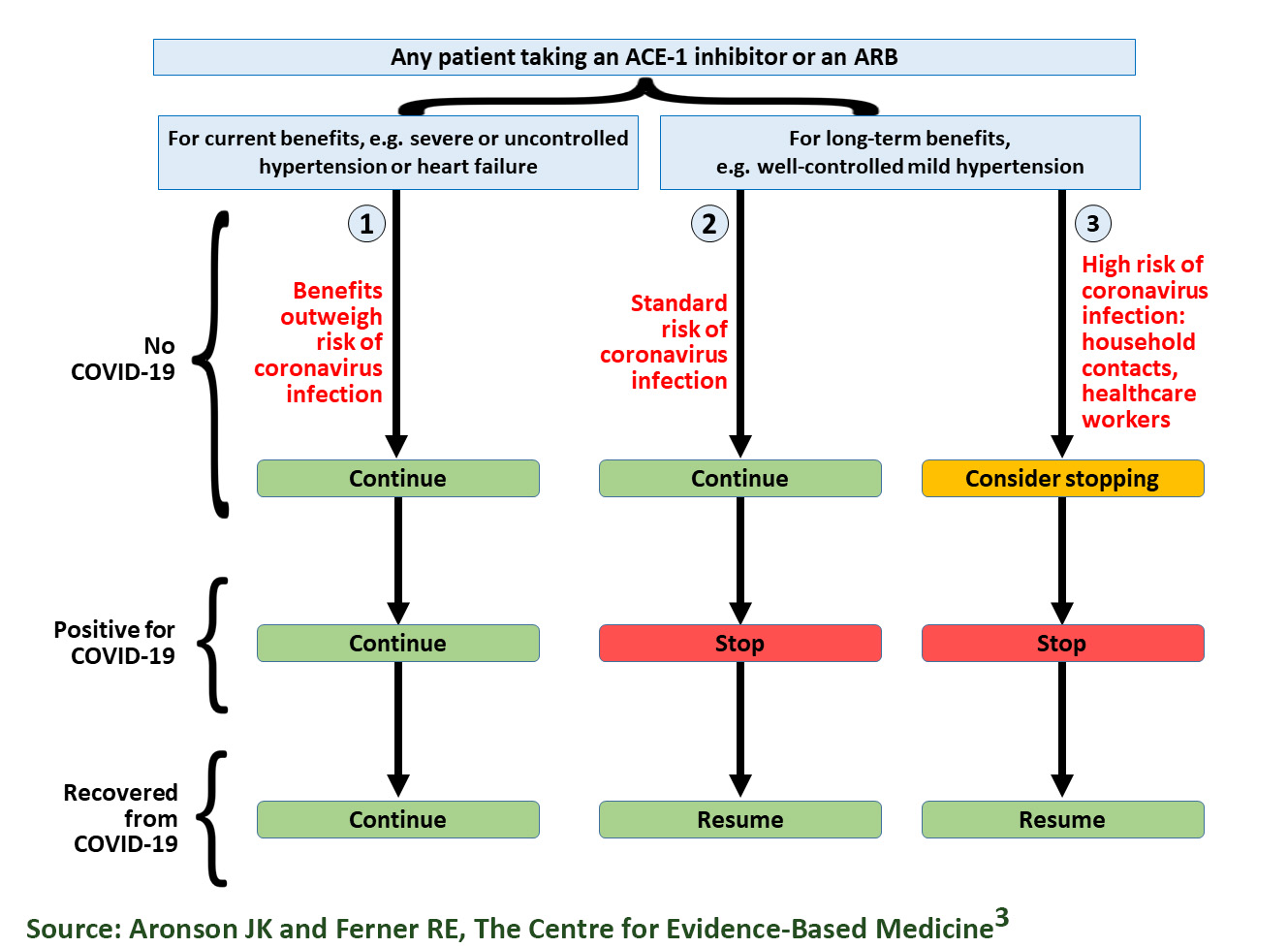
Health Watch USAsm Summary of Recommendations Regarding
ACE Inhibitors and ARBs with COVID-19.
Medscape: "Dr Fauci wondered why someone with well-controlled
hypertension would have a much greater chance of dying from
COVID-19. He urged delving into this deeper and finding out which
medications those individuals were taking."
https://www.medscape.com/viewarticle/928099He further stated:“If you look at the mechanistic rationale for concern, it is
there and it is firm.”
The below audio clip of Anthony Fauci, MD is from JN (JAMA Network)
Learning March 19, 2020.
https://edhub.ama-assn.org/jn-learning/audio-player/18324686
Additional Data on this was raised in the NIH Director's Blog:
“The genomic data of the new coronavirus responsible for COVID-19
show that its spike protein contains some unique adaptations. One of
these adaptations provides special ability of this coronavirus to
bind to a specific protein on human cells called angiotensin
converting enzyme (ACE2).”
https://directorsblog.nih.gov/2020/03/26/genomic-research-points-to-natural-origin-of-covid-19/
Some
articles have stated there are benefits to ACE inhibtitors which
have been shown in the laboratory. However, some of the
laboratory
research in mice used losartan (angiotensin II receptor
antagonist) with an acute exposure not specified, and may not be
adequate time for upregulation of ACE-2 receptor. In a prior
publication, only a 30 minute pre-treatment of the inhibitor was
used and the effect on ACE-2 receptor expression is unknown and
therefore long-term viral effect on the lung cannot be determined.
Future Therapies
One
research project which administered Recombinant Human
Angiotensin-converting Enzyme 2 to COVID-19 patients has been
withdrawn due to unfavorable results in a pilot study (Clinicaltrials.gov #NCT04287686) and a
blocker of TMPRSS2, camostat mesylate, has been approved for
human use in Japan for another indication.
This webpage is for guidance only,
always consult your healthcare provider and the
CDC Website for information before making decisions relating to
the coronavirus.